Back in January 2021, Phillip Alvelda issued a warning. Alvelda is a former NASA & DARPA technologist-turned-entrepreneur who runs Brain Works Foundry Inc. and Medio Labs, U.S.-based developers of A.I. enhanced health care technologies and services. He said that a new variant of COVID-19 would spell disaster without a change in mindset and a rapid, robust response. Today, as several U.S. states experience some of the worst outbreaks on the planet due to the delta variant, Dr. Alvelda sounds the alarm that the calculations for beating the pandemic have changed and we need to catch up. He explains to Lynn Parramore of the Institute for New Economic Thinking that while vaccines must be the foundation of our response, additional measures are required to prevent ongoing – and unnecessary — suffering and death.
Lynn Parramore: Why is it wrong to think of the delta situation as “just another surge”?
Philip Alvelda: We have quite a lot of information from all of the countries that have been beset by the delta variant before us. It began in India and was transmitted very quickly to India’s close trading and tourism partners. The U.K., of course, was one of the first affected by the new wave, but it hit broader Europe – France, Belgium, Portugal, and Spain, and so on. Israel was hard hit as well. So, we have data on the expected course of the disease, the number of people an infected person transmits the virus to, and so on. We have laboratory data that show how even a completely vaccinated person – someone with two doses of the Pfizer vaccine – sheds as much virus for the first six days as someone that hasn’t been vaccinated. We can see that with delta, the disease ramps up substantially faster in the body when you’re infected than the original Wuhan strain, where it used to be four days before you would become infectious and could spread the disease to others. With delta, you can ramp up from the point where we can just barely detect the virus with our best PCR test all the way to full infectiousness within one day.
If you take all of those things together, you realize that this strain is quite a bit more problematic to contain. We’ve watched these other countries go through the process of realizing exponential growth in the disease — faster than we’ve ever seen it before. We also see that the old abatement measures worked up to a point and then just started to fail. These countries have had to do more than they were doing before to contain the virus. So it’s definitely not “just another surge.”
LP: In the U.K., many have felt hopeful that the pandemic is under control after a rapid rise in delta infections was followed by a significant drop. Others note that the virus is unpredictable and cite indications that case numbers are ticking back up. What’s your view?
PA: When we look at the reasons for the change in the trajectory of delta in the U.K., we see two really big changes that heralded the peak. One was the end of the Euro soccer tournament, which we know was a whole series of superspreader events. We know how many young men had caught the virus by the end of the matches and so on. That tournament ended just prior to the decline in cases. The other thing that happened right before the decline was that school was let out, so no more in-person classes. The schools were a huge spreading agent. We’ve now tracked the variants and the disease prevalence by age, and it’s clear that the school-bound cohorts spread the virus like crazy before school ended, and then when school ended, cases in that cohort starting to decline rapidly. So we know that the Euro games and the school closings were the big things that had an immediate effect. But school is coming back into session and they’re continuing to have additional soccer games, although not to the same extent as the Euro finals.
Unfortunately, we can actually see in the numbers over the last week that the U.K. is back to exponential growth of the delta variant. So far, it’s relatively modest exponential growth, but still exponential. This is not speculative. It’s happening.
LP: So we can say with certainty that the U.K. is not out of the woods?
PA: No, it isn’t out of the woods. Looking at the different age cohorts and looking at the different regions in the U.K., you can see that the decline was not universal. There were some demographics where you had broad decline like the schools, and others which were flat, and now we’ve got a whole set of them that are increasing once again.
LP: You note that vaccines are currently working very well for personal protection, with far less hospitalization and death for vaccinated people who contract the delta variant than those who are unvaccinated. But you warn that current vaccines no longer work well enough for public health suppression of delta. What exactly does that mean?
PA: With a pandemic, if you allow the virus to continue breeding in meaningful amounts, you’ve got big problems. If you let the disease kind of run its course through a large part of the population, and there’s this churning aspect of many, many people carrying the virus and allowing it to breed and mutate, then just by selective pressure, the virus is developing new generations that can potentially survive the vaccine. We are running a giant experiment. Some epidemiologists will say that if you wanted to design a super-virus, you’d do exactly what we’re doing right now – you’d vaccinate half the population to apply the selective pressure, and then otherwise let the thing keep growing and mutating so it learns to avoid the vaccine.
LP: What do you say to the pervasive view that delta is really just a problem for the unvaccinated, or for people in red states. Is that accurate?
PA: The new delta variant really changes the equation. Two things are coming into play simultaneously. The vaccines were designed to target the original Wuhan strain from over a year ago, and they don’t work as well against delta. Although we have high vaccine efficacy for hospitalization and mortality, and this is very good news, the vaccine efficacy for catching the virus and carrying it and retransmitting is not as good, like 80%. In fact, Israel claims it’s as low as 60% for their mix of vaccines.
LP: So even if we live in a blue state with large vaccinated populations, we still have a problem because delta is still spreading and getting a chance to mutate into possibly even more dangerous variants?
PA: Right. And there’s also the problem of long-haul Covid, which you can get even if you are vaccinated and have a breakthrough case. Even if your case was asymptomatic.
LP: A lot of people still seem dismissive of long-haul Covid, even though recent reports say that one in four Americans who contract the coronavirus get long-haul symptoms, like shortness of breath, debilitating fatigue, brain fog, and memory loss. Keeping in mind that the delta variant is still relatively new, so much remains to be seen about its long-term health effects, what do we know so far?
PA: Fortunately, we’ve got data from the U.K., which is much better than anything we’ve generated in the U.S. The challenge in the U.S. is that we’ve failed to get a large-scale testing program that tests everyone regardless of whether they volunteer, have symptoms, or not. The data that we have from the U.K. includes everyone. It’s a good random sample of the population of people that have Covid and know it, those that have Covid and don’t know it, and the people that don’t have Covid but might have other health issues.
In the U.K. there has been amazing statistical analysis of that data, which show a couple of really important things that are very different from what the sparse data that we have in the U.S. show. In the U.S., you see these tweets from physicians that say that fewer than 1% of the population shows any long-haul Covid issues. Well, the problem is that people are not being identified as having long Covid issues because they aren’t being tested — so they don’t understand that the issues they are having are related to Covid. But in the U.K., where they’ve done these massive surveys with hundreds of thousands of people, they actually can show that yes, long-haul Covid is a serious issue, and not just for the unvaccinated. It’s affecting everyone. Anyone who has the disease, whether they have symptoms or not, actually has a reasonably high likelihood of having one of the symptoms that persists long after the infection.
LP: So just to be clear, even if I’m vaccinated and my infection was asymptomatic, I could end up with problems that last for months if not longer?
PA: That’s correct. The challenge is that these issues are so hard to identify. When you get Covid, it attacks the ACE2 receptor, which happens to be all over your body. So when you get a Covid infection, it could establish itself anywhere – your brain, your lungs, your intestines, your stomach, your joints, your muscles, and depending on where it really takes hold in different peoples’ bodies, you can have a vast array of different symptoms that are a result of the damage that the virus does to that part of your body. The effects can be muscle pain, indigestion, brain fog, cognitive difficulties, muscle spasms, all kinds of things that we now know are due to Covid. And it’s only when you do these broad survey questions that you can catch them and realize, oh, your muscle pain isn’t because you’ve been playing football, it’s actually because you had Covid.
LP: What concerns you the most with long-haul Covid?
PA: Unfortunately, we have to deflate the false sense of security that we’re going a good job with the pandemic and we are protecting people who are vulnerable. Right now, we don’t have the proper measures in place. The real menace is the people who are promoting “just learn to live with it” policies and really turning our children into an experiment for a systemic disease that we know does serious damage and can have effects that last a long time.
We’re gathering more and more data, and it’s most painful for me to see it in the children. In places like the U.K., Canada, and Florida, unvaccinated children are being sent to school with poor abatement protections. In Florida, something like 7,000 children contracted the disease within the last four days last week. That means that there are going to be 700 or so of them that have long-haul Covid symptoms that could keep them out of school for months. And keep in mind that with delta, you can get Covid even if you’ve been vaccinated. You can still have massive viral loads and you can still have long-haul Covid.
LP: And yet we still have people out there saying that Covid is just like another flu. How does the delta variant compare to the flu?
PA: At a stretch, you might have been able to compare the flu to the Wuhan variant, but delta is so much worse. It has a thousand times the viral load and twice the ramp-up speed – meaning that when you contract the virus, you become infectious to others much more quickly than you do with the older variant. Delta has higher mortality and morbidity. We need more data on long-haul Covid with delta, as you say, because it hasn’t been around long enough. But anyone who says that delta is not a long-haul Covid threat is fantasizing, I’m afraid. You take something that is as transmissible as chickenpox, where you can expect one infected person to infect between seven and nine other people, something more than ten times deadlier and nine times more infectious than the earlier strains — it’s a big deal.
LP: Why do you say that vaccines alone can’t stop the pandemic? What else do we need?
PA: For you personally, vaccines offer strong protection from delta for both hospitalization or death, but as we’ve just discussed, you may not have protection from long-haul Covid. And in terms of getting the virus and passing it on, the effectiveness is not so good. It’s important to understand that the vaccines were very good and effective to start, it’s just that they were targeting an older variant. We’ve been too slow on vaccine distribution and we’ve got too many antivax influencers. We just haven’t vaccinated enough people. The combination of not getting to a decent vaccination threshold and having the vaccine efficacy drop as the new variants emerge means that right now we’re not going to get enough suppressive effects of the vaccine alone to slow and stop the transmission.
LP: Let’s talk about herd immunity. There seem to be more and more scientists saying that we may have trouble getting to herd immunity with delta. What’s your take?
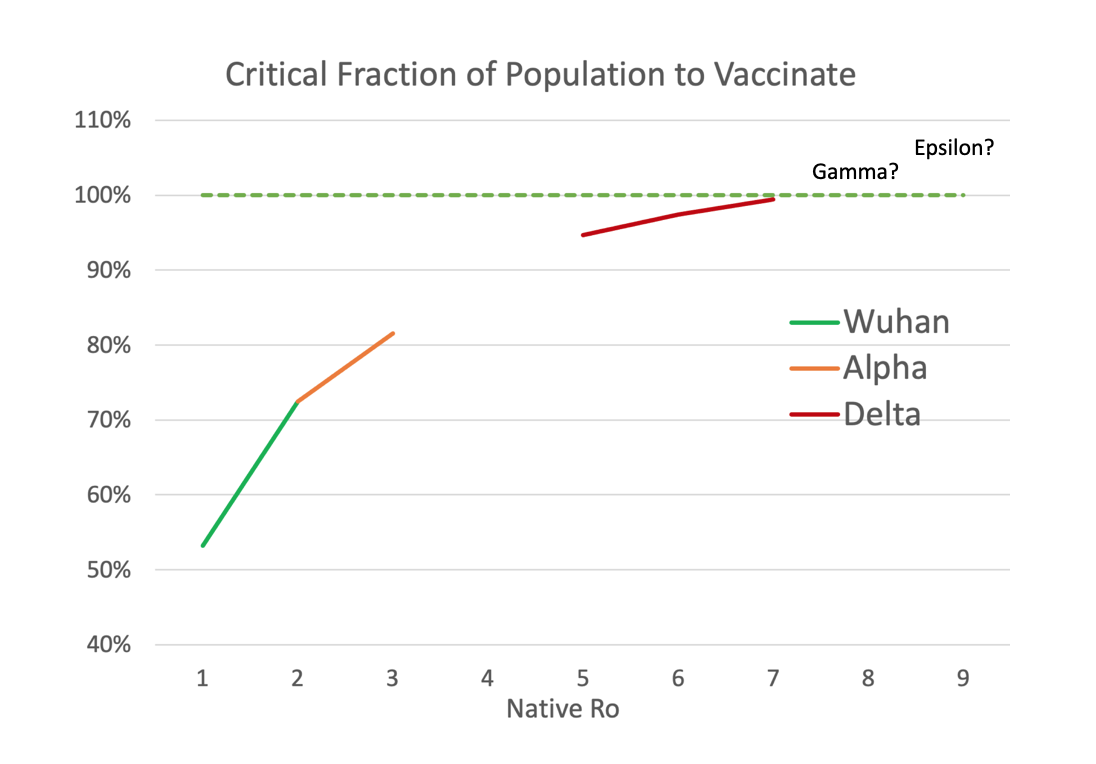
PA: Well, we never got to herd immunity with polio or smallpox. We had to learn how to eradicate them with aggressive and universal vaccine campaigns. I do think that herd immunity is similarly possible to achieve with Covid and that there are nations that are going to do a decent job of it. But they require a few things to happen. The vaccines need to be administered quickly enough that you vaccinate enough people to suppress the virus before it has a chance to mutate out from under that vaccine’s protection. To really suppress the virus quickly, you need to use additional means so that it stops mutating into new variants. The whole effort of designing the vaccine, having it approved by the regulatory bodies, distributing it, and getting the population to start taking it — that all has to be faster than what we’re doing. It turns out that the speed of response against these viruses is really critical. I think many people don’t fully understand how high the immunity threshold needs to be when you have a virus that’s so infectious.
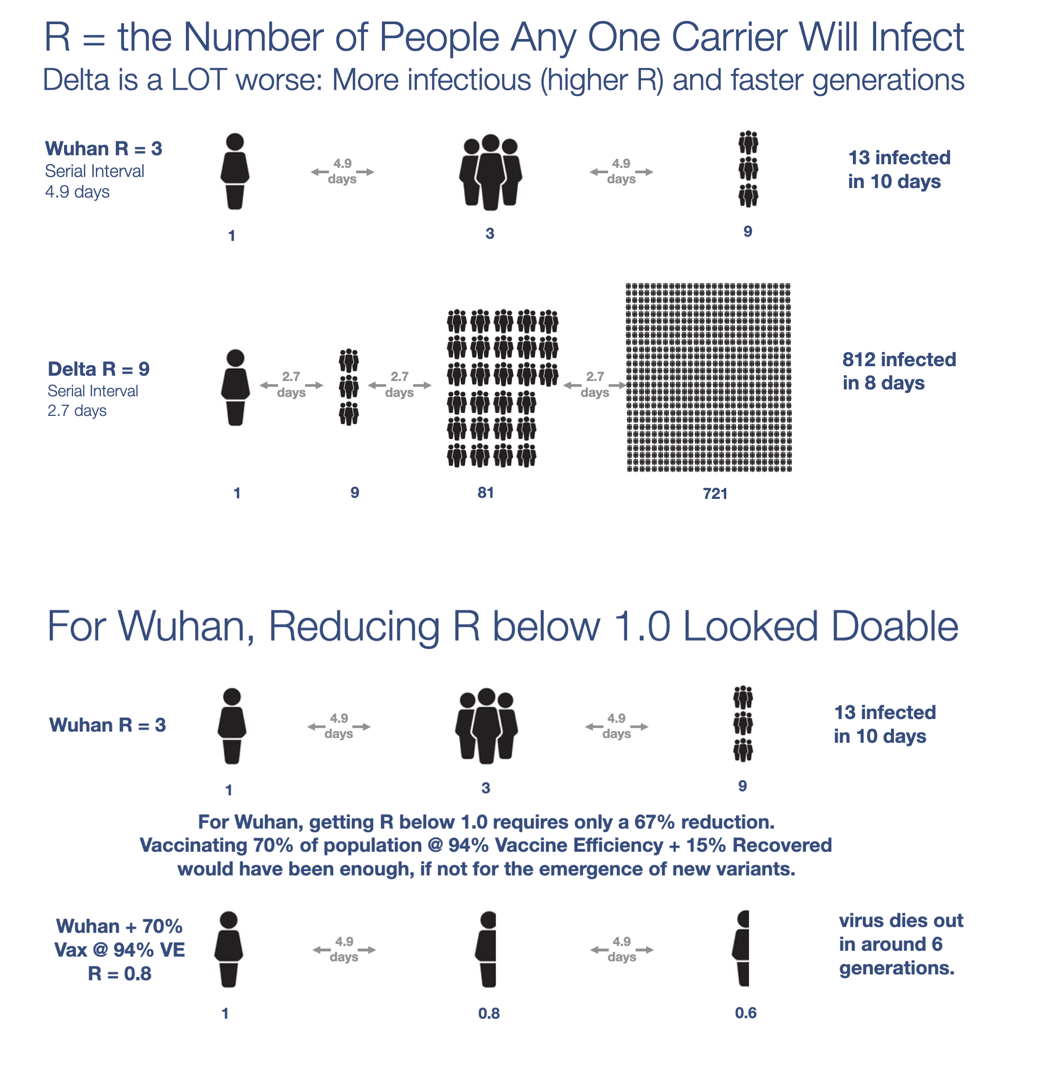
Scientists talk about something called the R number. The R number is a way of rating a disease’s ability to spread. R really tells you how many people you expect an infected person to infect. When R starts somewhere between 7 and 9, as it has for this delta variant, we need to be having about 95 to 97% of the population immune in order to achieve herd immunity. Once you’ve been vaccinated, you have pretty good immunity for the first six months, but then it starts to drop at about 3% per month. The longer you wait to kill the new variants, the less you’re protected from the last time you had it. We have this problem of declining efficacy both in having it and being vaccinated. That’s why the CDC is now talking about giving everyone boosters.
LP: So herd immunity is a race.
PA: That’s exactly right. What makes it particularly hard is that these waves of the new variant come and go exponentially. The problem with our vaccine responses is that they’re linear. I can add a fixed number of new hospital beds. I can ship a fixed number of new masks. But the delta variant is doubling every ten days. When the prevalence is limited, you can mount a good response early. You can ship the masks, have the mandates, and distribute the vaccine, but once you’ve got a reasonable spread and exponential growth really kicks in, everything becomes a real struggle.
LP: What tools do policymakers need?
PA: There’s a whole set of states that need to apply science-based policy to combat the virus rather than just letting it go. The truth is that they will inevitably learn to do so when it gets bad enough, because if you don’t stop the exponential spread, eventually your hospitals will be overwhelmed. Sadly we’re seeing that now in Arkansas, Texas, Louisiana, Florida, and many more states are on track to do the same. So this narrative that it’s a red state pandemic is not true. Cases are growing in 48 states and are on their way to overwhelming their hospitals – Republican and Democratic-led states alike.
We need to realize that when we haven’t vaccinated enough people and we’ve waited too long, where the vaccines are less effective than they could have been on the older strains, the vaccines alone are not going to be enough on their own to slow this disease. We have to reinstitute abatement measures on a national scale. That means masking, distancing, limits on capacity in bars and restaurants, and large-scale surveillance testing. Doing those things in combination with the vaccines, we could actually slow the thing down. But trying to rely on the vaccine alone or, even worse, avoiding the vaccine, means that the virus is going to continue breeding new variants that get more contagious and more infectious.
LP: Do you see more lockdowns in our future?
PA: I empathize with people who say that we don’t want to have a lockdown. I don’t want to be in a lockdown, either. But there are things you have to do if you want to avoid it. You’ve got to stop the exponential growth by other means.
The most important policy tool in that regard is fast action. You’ll see the difference between California and New York, for example. Though they waited longer than I would’ve liked, they acted in the first four to five weeks of the exponential growth of delta. Other states have waited until the pandemic has gotten as bad or worse than it ever was before to take any extra action. Then you have some states, like Florida and the Texas governor, who are actually preventing other measures. These people who say they want to avoid masks and social distancing mandates, and they aren’t going to do a lockdown, well, they’re guaranteeing that they’re going to have to do lockdowns because they’re not addressing the virus early enough where milder measures could have prevented a more severe situation with hospitals being overrun.
LP: Is it fair to say that the anti-vaxxers and Covid-deniers, despite their rhetoric about not wanting to be vaccine guinea pigs and their vociferous objection to lockdowns, are actually turning us, particularly our children, into guinea pigs for this mutating virus and creating the conditions for lockdowns?
PA: Yes, it is. We have a few really important challenges in the U.S., but there’s a lesson that’s going to sink in at some point: the idea of divide and conquer. That means when you get an area clean, you keep it clean. And that means border controls. We haven’t really had border controls between the states until this pandemic. The CDC just added France to the “Do Not Travel” list for U.S. travelers due to Covid. Well, guess what? It’s worse in Florida than in France. It’s worse in Texas. It’s worse in Louisiana. Probably in 15 or 20 states already. So shouldn’t the CDC add the “Do Not Travel” recommendations to those states?
LP: How do you enforce that?
PA: It is difficult to enforce, but at least you could slow things down, preventing planes and trains from coming in, and so on. But it’s pretty clear that some states are going to continue sustaining the virus while others continue to try to fight it. Some are fighting it effectively and others aren’t. Just watch over the next couple of weeks the difference between Louisiana, Texas, and Florida, and New York and California. The surges in the faster-acting states will be shorter and cost less. The others will take longer to deal with, cost more, and kill more people.
LP: Between vaccines alone not being enough to halt the spread of the virus and Long-haul COVID, what does this mean for all the schools that are rushing to open for in-person instruction, some with no vaccine or mask mandates at all?
PA: Remember what happened last year, when the schools rushed to open without the proper mitigation measures in place for the Wuhan strain. Those schools that made the attempt when the virus was even at moderate local prevalence immediately had outbreaks in the school and accelerated the growth of the virus in their communities. When the exponential growth wouldn’t abate on its own, they had to shut down in-person instruction and go virtual.
Before they had the vaccines, those schools that were successful in remaining open used masks, distancing, and improved ventilation along with regular surveillance testing to keep the virus out of the schools and minimize the number and duration of outbreaks.
But now, the stats and risks with delta are much worse. So much so, that students are in a worse situation now, even with about 50% of the U.S. vaccinated, than they were with Wuhan last year. With the delta variant and no abatement whatsoever, an infected student or teacher would, on average, infect nine other people!
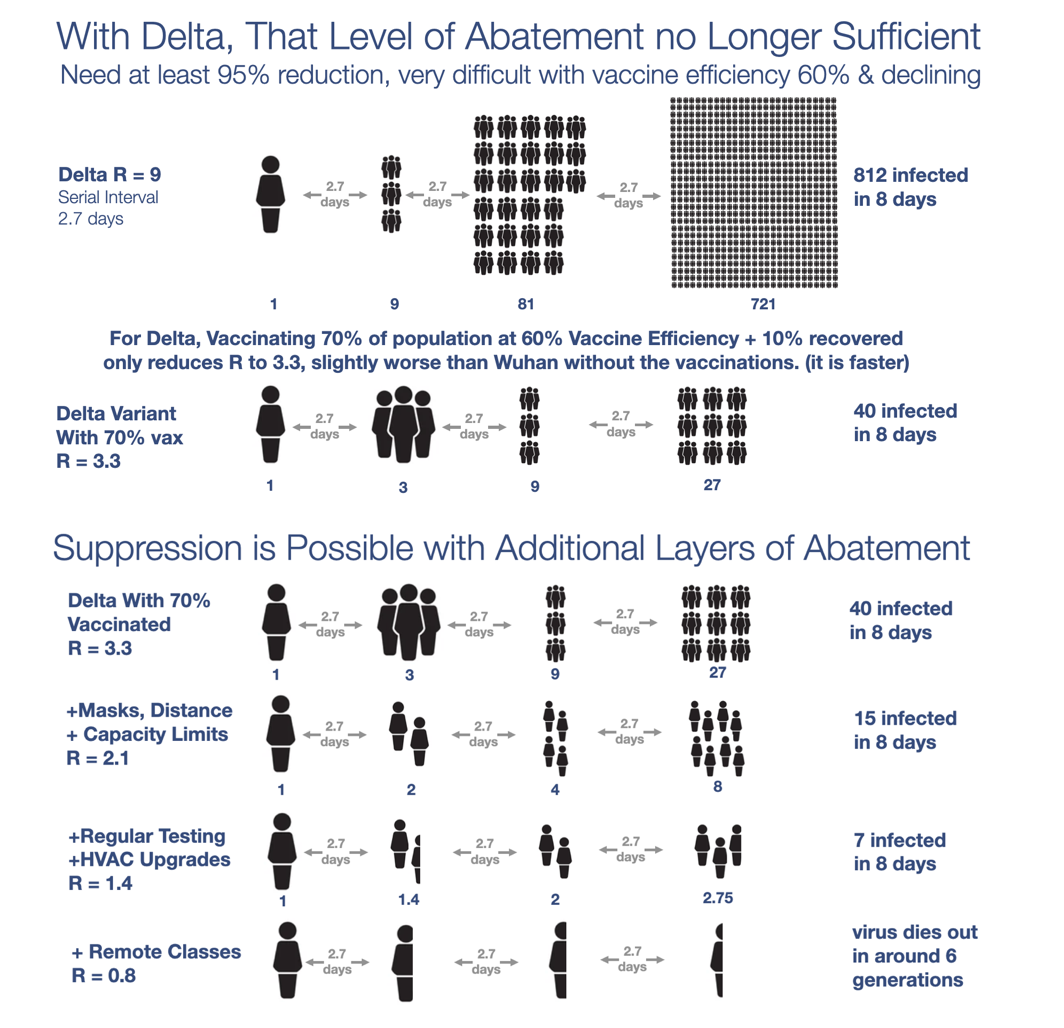
Even if your school community was vaccinated at the average U.S. rate of about 50% with a 60% vaccine efficiency versus sickness and retransmission, that just means that an infected person would infect at least five other people instead of nine, and the virus will continue to grow exponentially.
The good news is that if you throw in regular surveillance tests, masks, and improved ventilation and HEPPA filters, you can take the number all the way below one and suppress the virus.
Schools essentially need a multi-layered defense strategy or risk mass outbreaks worse than in 2020. Sadly, early reports from the first partial weeks of school are already sounding dire, especially in those states eschewing any meaningful measures. One Tampa, Florida district reported 5,599 students and 316 staff quarantined after the first four days of school.
LP: What can parents do?
PA: Enough of the states are having problems that it really doesn’t matter where you are at this point. The number one thing is to get kids double vaccinated with one of the mRNA vaccines. With the younger ones, take them the moment the vaccine is approved for them. And keep in mind that because vaccines are not an ultimate protection as they once were, look for a school that is going to take abatement measures seriously and recognize the fact that asymptomatic people can spread the virus and that having a vaccine doesn’t prevent you from spreading it.
Besides the masks and the distancing, the schools really have to have proper ventilation, filtering, and air exchanges. We know that the virus is airborne and that the primary path to infection is through aerosolized droplets. We’d like to see much more attention and understanding from the CDC, OSHA, and anyone who writes policy for the schools, that the virus behaves like cigarette smoke. It’s not really about droplets or contracting the virus through contact. If you’re indoors and the windows are closed, six feet and masking won’t work. The room gets filled with the virus. Plexiglass can even trap the virus and increase your chance of getting it! You want the air exchanged rapidly and you want particle filtration that will use a HEPA filter to capture the virus particles.
Fortunately, there are easy ways to test how well you’re doing. You can get a $200 CO2 meter which you can place in a room and track how much CO2 is gathering. That’s a measure of how much air has been exhaled by other people. If the CO2 level goes up, your risk goes up. This is very low cost. Any school can afford a gadget to take through the classes through the course of the day and measure how they’re doing.
Bottom line, if you don’t feel like the school is protecting your children, find another school or keep them at home.
LP: Your company has been working on low-cost, high-sensitivity Covid tests. If the delta variant ramps up faster in the body, becoming infectious to other people more quickly, does it mean we need more than the once-a-week testing that has become common in schools and workplaces?
PA: Once a week is the bare minimum of what you could do for the Wuhan strain. That’s when the virus took four days to ramp up to infectiousness in your body. Now, with the faster-acting virus, you need to be tested two or three times a week. Ideally, you would have a three-times-a-week test with very high sensitivity to detect the virus as early as possible. You have very little time to detect it before people start spreading it. You need to catch it when the virus is still at a low concentration in the body. Unfortunately, a lot of the rapid tests and antigen tests in use now are not that sensitive, in which case you really need to do daily testing.
LP: Is there some good news to leave us with?
PA: The good news is that the new mRNA vaccines really are scientific wonders and are the single most powerful protection anyone can muster. So go get that and feel 80 times safer from death or hospitalization. Also know that we’ve seen places like New Zealand, Germany, and Singapore manage to get delta under control with diligence in applying new measures in addition to the vaccines. They instituted strong mask policies, distancing, capacity limits, and so on. This is doable. We should absolutely be able to do it ourselves if we can get ourselves a little more science-aligned and a little more unified and cooperative in battling the virus instead of each other.