
The scale of disaster visited on the world by the COVID-19 pandemic defies any easy summary. But it is safe to say that the question of keeping schools open is among the most fateful decisions facing public authorities. As the pandemic stretches into its second year, it is now becoming among the most contentious.
In the U.S., after some hesitation, the Biden administration seems to be encouraging rapid opening of schools, despite high levels of community transmission in many places, before robust mitigations are completely in place. Many Republican governors and officials also demand the step, including former President Trump in his recent CPAC address. Languishing under lockdowns and zoom or hybrid classes, many exhausted parents, anxious employers, and bored students seem receptive, though polls show widespread reservations about whether premature reopening might trigger new waves of infections. In recent days, more and more states have moved to mandate full in-person classroom instruction within a few weeks.
Accompanying these decisions are organized efforts to recycle earlier studies of school safety[1] designed to reassure skeptics that reopening schools to full-time instruction is really safe, even as new variants of COVID-19 spread that are more contagious and possibly more dangerous than earlier forms. Even the Center for Disease Control is joining this rush to judgment, suggesting that seating students as little as three feet apart might be an acceptable rule for social distancing.
Bitter experience has taught us a great deal since the beginning of the pandemic. Among the most important lessons we have learned is that it is not, in fact, safe to open schools as the pandemic persists without close adherence to significant and stringent abatement measures.
We begin with the most important point as to how we now better understand the risks that eluded us in prior surges of the virus. In those earlier episodes, many people who in fact had the virus showed few indications that they did, even as they went on to spread it to others. This “asymptomatic” transmission was a genuine novelty that researchers only slowly came to grips with.
Unfortunately, the display of coronavirus symptoms is highly correlated with age, thus the younger the student, the less likely they are to show symptoms, or exhibit what are considered “typical” COVID-19 symptoms. The younger students, therefore, were much less likely to be tested. So they continued participating in the school community even as they spread the disease and even having suffered symptoms and long-term side effects that absent a COVID-19 diagnostic determination, were falsely attributed to other illnesses. As a result, the studies commonly cited as supporting school reopening are deeply flawed; they are based on having only tested students who showed symptoms, rather than applying broad screening tests either universally or with true random samples capable of catching the otherwise undetectable asymptomatic spreaders and infected.
The extent of this bias has now been quantified in several studies in the UK, such as the Office for National Statistics Infection and Household Surveys[2] and REACT-1 Studies.[3] These studies randomly sampled large numbers of households within the UK at regular intervals regardless of symptoms. The results are dramatically different from the earlier studies, and even from symptom-based testing from the UK during the same time period; they show that contrary to the conclusions from earlier studies based on biased symptom-only testing protocols, in-person schooling is associated with much higher risk than previously thought. A recent study published by the Center for Disease Control (CDC) from Mississippi confirmed these findings; it showed that case-based reporting of infection in children underestimated infection by between 14-68-fold over May to September 2020 compared with serological surveys.[4]
With the more recent large-scale random sample testing performed in the UK, Sweden, and the US, we now know the following facts:
1. The secondary COVID-19 attack rate – that is, the rate at which the coronavirus spreads – was actually higher for both elementary and high school students than adults when the schools were open for in-person instruction between April to November in England (ONS Household Infection Survey).[5]
2. Both elementary and high school children were far more likely than adults (2x and 7x, respectively) to be the first case in their households rather than the adults between April-December in England.[6]
3. The spread of infections among school-age children and in the community closely tracked school openings and closures as well as attendance, with the prevalence of infection being highest in these groups compared to all other age groups while schools were open and tiered restrictions for broader society remained in place. Importantly, particularly with the new variants, growth of the pandemic continued in regions where these variants were prevalent even as other institutions were shut down in the national lockdown in November.[7] These statistics were mirrored in a recent study on the risk of coronavirus spreading in U.S. schools.[8]
4. Increases in the prevalence of infection among school-age groups preceded rises of infection in other age groups. This has a vital implication; the new studies suggest that infections among children at school do not just reflect infection rates in the community. Rather, they drive increases in infection within the community through spreading from schools into homes, and from there to the broader community.
5. Claims that teachers do not face serious risks are simply false. The risks of infection turned out to be two times greater for teachers of in-person classes relative to those conducting virtual online classes in Sweden.[9] The study also found an approximately 40% higher infection risk in England in those in teaching occupations compared to those in non-teaching occupations, even when schools were only partly open (REACT-1 study).[10]
6. Several studies also show an increased risk of infection among parents of primary and secondary school children being taught in-person within schools.[11]
7. The spread of new, more easily transmitted and more deadly variants underscores the true dimensions of the threat from in-person school instruction. With the new B.1.1.7 variant now surging in many parts of the world, variant cases continued to rise with an R=1.45 (compared to an R of only 0.9 for non-B.1.1.7 variants) even during national lockdown while schools were open. R only dropped below 1 – a critical level for controlling the rate of infection – following complete school closures. The numerous outbreaks linked with B.1.1.7 in school settings across the globe over the past few weeks are of grave concern.
8. Between 12-15% of primary and secondary school children had one or more persisting symptoms 5 weeks after infection, according to an ONS survey that took care to examine all infections, including asymptomatic infections.[12] Before that study appeared, it had been widely thought that because mortality is low among children exposed to SARS-CoV-2, that children are not impacted. Given we know so little about the long-term implications of “long COVID” syndromes, which at least in adults have been often associated with organ dysfunction, it is important to adopt the precautionary principle, and reckon with long COVID related outcomes in addition to deaths.
9. Recent evidence supports the role of mitigations in reducing the impact of transmission within schools. However, it is clear that multi-layered protections are needed, rather than single or a few measures, as the risk reduction is associated with the number of mitigations in place.[13]
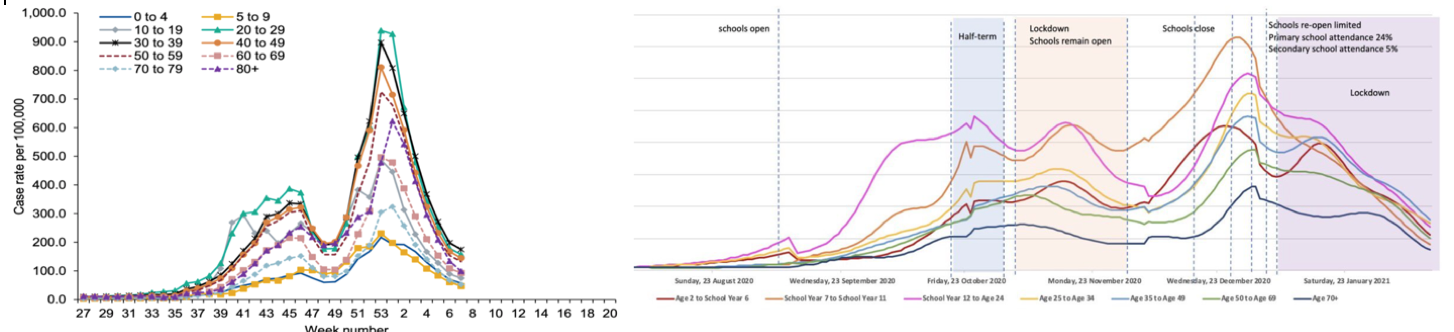
Figure 1 On the left is a graph from an earlier study based only on testing symptomatic U.K. patients that seemed to indicate that children aged 0-19 were the least likely to be infected or carriers of the coronavirus. Such symptom-based data from children are still being used to promote the notion of sage school reopening. The graph on the right shows the data from the large scale ONS study based on random sampling of households across England.[14] The latter study catches the large number of asymptomatic carriers, showing clearly that when asymptomatic carriers were counted, those school-age cohorts were, in-fact, the most likely to be infected carriers of the coronavirus. The ONS study also shows the correlation of new case growth in the elementary and high school-aged cohorts with times when the schools were opened for in person instruction and declines over vacation, half-term and shut-down periods.
The coincidence of the rush to reopen with the spread of the new variants of concern to the CDC and the World Health Organization is particularly unfortunate. The new B.1.1.7 variant is both 50% more communicable, and about 30% more lethal than the earlier strains. It is now the dominant and resurgent strain across Europe and is now endemic across the United States. All through the pandemic, the United States has lagged in testing for the virus. It has trailed not only in sheer volume but also in the form of testing: most tests cannot sort out the new more dangerous variants from older forms of COVID-19. Only so-called “genetic survey” tests can do that reliably and they are used only in a few places.
Data from the relatively few U.S. states that use these viral genome survey tests strongly indicate that the now widely reported declining case numbers mask a dangerous, exponential rise in cases of the newer more contagious variants. These appear even now to be turning around the recent falls in total cases in some areas of the country. We expect that in the next few weeks that phenomenon will show more widely.
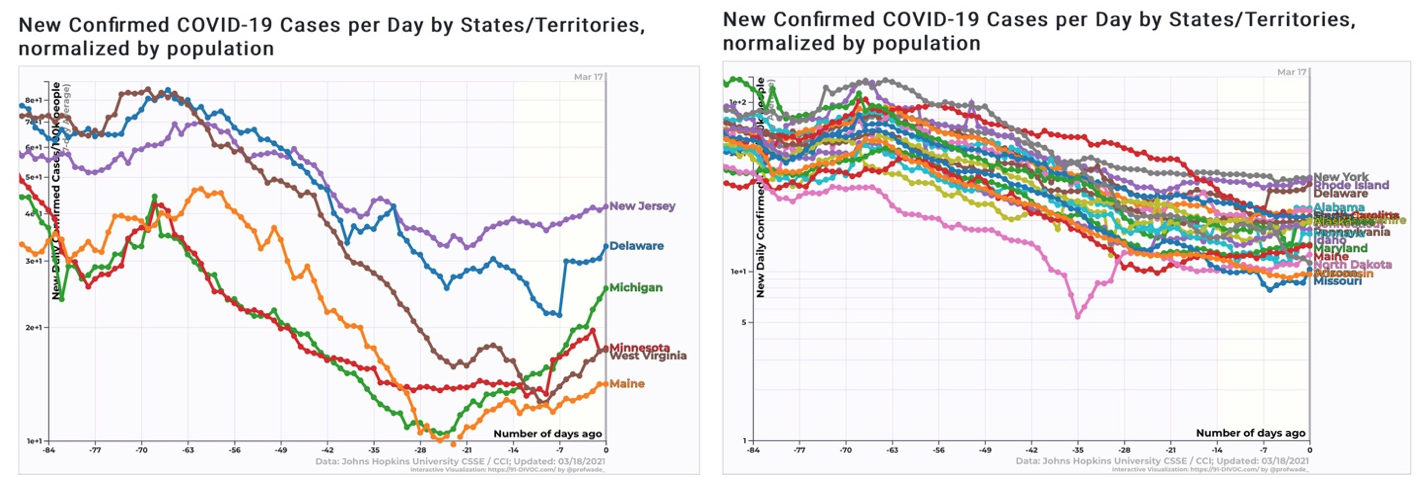
Figure 2 After months of steady decline, we can now see the return of significant growth in new COVID-19 cases across six states where the B.1.1.7 strain is known to be growing in prevalence. Cases are now flat or starting to rise in 21 additional states, and we expect resurgences soon there as well. Relaxation of abatement measures is clearly premature.
Another lingering concern testifying to the persistent impact of outdated science is that so much of schools’ reopening guidance remains aimed at hygienic measures, surface wipe-downs, and plexiglass barriers, all of which are completely ineffective in limiting what we now know is the primary mode of indoor transmission, airborne aerosols.[15]
The latest CDC guidance suggesting that the risks to students are similar at 6 foot or 3-foot distances and thus that schools can safely reopen with more-or-less normal student seating density and populations in the classrooms completely misses the point. A close analysis of the “3-foot paper[16]” the CDC cited shows it to be riddled with errors in protocol, most importantly, that it again relies on data from primarily symptomatic carriers; that it improperly conflates infectious susceptibility with contact rates; and is based on a flawed sampling methodology.
Neither did it measure the actual distancing practices within classrooms, but rather considers guidance at district levels, and only for all schools with attendance greater than 5%. This could mean that schools were wrongly categorized to different distances that were not accurate. Differences in other mitigation measures, class size, or class attendance were also not accounted for. Ultimately, the study is also too small to come to any scientifically supported conclusion, as the results show that the risk of infection among districts with guidance to distance greater than 6 feet could vary from half of those with guidance to distance greater than 3 feet by up to 1.3 times as much.
Most critically, while the authors were correct in saying that there is little difference in risk relative to seating distance, they drew exactly the wrong conclusion from the distance data. Newer science has demonstrated quite definitively that the coronavirus spreads heavily through the air, more so, in fact, than through droplets on surfaces or direct contact. As a direct result, the earlier 6-foot indoor social distancing rule guidance was proven to offer misleadingly false comfort wherever ventilation is poor. A beautifully illustrated and simulated interactive New York Times article highlights “Why Opening Windows Is A Key to Reopening Schools” safely. It’s worth a read, because it also demonstrates clearly why relaxing distancing measures, say to seating students 3 feet apart instead of at a 6-foot distance is not necessarily a good idea.
Contrary to the notion that even 3 feet of distancing is sufficient protection, and 6 feet is overkill, the critical safety issue is that students are all uniformly at risk in poorly ventilated rooms no matter where they are or how they distance. With one infected person in an enclosed and poorly ventilated room, the coronavirus permeates the entire space, putting everyone inside at similar risk regardless of where they sit. The key corrective abatement measure necessary is wholesale improvement in ventilation, filtering, and HVAC systems. Nothing whatsoever in any of the cited studies supports safely moving students closer together.
The Biden administration’s new emergency aid bill contains substantial funding, at last, for states and localities. They could use some of that money to refit ventilation systems in schools and implement rigorous testing programs, and even quickly roll out portable HEPA filter systems. But as of 2020, a GAO study indicated that ventilation and heating systems in slightly under half of the school systems examined required substantial new expenditures to meet code, much less enhanced protection necessary for coronavirus abatement. With substantial federal support only now coming available, properly replacing older ventilation systems with HEPA filters will take time.
And though rapid COVID-19 tests are now available, few public schools can afford the current generation of tests. The simple mathematics of exponential growth and airborne transmission in confined areas means that tests on everybody – students, teachers, and staff, including cafeteria workers and janitors – need to be performed at least twice a week. Testing less often means that the virus cannot be identified fast enough to stop outbreaks from sweeping through schools and that contract tracing and quarantine efforts come too late to be effective. And similar to the HVAC upgrade concern cited above, it will also take time for forthcoming federal aid to flow down to schools and labs to enable frequent and affordable school testing on a national scale. In any case, these tests should not replace robust mitigatory measures within schools, but rather complement a robust, multi-measure mitigation approach.
A reconsideration of the current rush to reopen in-person instruction with less than sufficient mitigations is, therefore, clearly necessary. The understandable hopes for a return to normalcy raised by the stepped-up campaign to vaccinate everyone are premature. The vaccine effort, while gathering momentum, will not reach enough people quickly enough to make opening this Spring safe, without more robust mitigation measures within schools. And the costs of making a rushed mistake based on outdated science will take too long to become obvious.
We understand and sympathize deeply with the pain that the continued delay of reopening causes our colleagues and fellow citizens. But it cannot make sense in the actually existing state of most public schools (or, for that matter, all but the most affluent private schools) to push to reopen without all the critical mitigations, as this will once again potentially lead to educational disruption in the form of school closures and further lockdowns. Better to ensure schools can remain open once they do restart through robust mitigation, ramping up testing, ventilation, and, above all, vaccinations than send new waves of sick students, teachers, and parents to already overstretched hospital and emergency medical facilities in a third resurgence of the coronavirus, and unnecessarily put a generation of students, teachers, and parents at risk of Long COVID side effects.
Reopening most schools now, before most schools lack robust protective measures, and don’t yet have broad ability or finances to conduct frequent surveillance testing to prevent asymptomatic spreaders of the latest, more dangerous coronavirus variants from infecting their community, is thus very unwise.[17]
Notes:
[1] Bailey, “Is it Safe to Reopen Schools,” CRPE
[2] Coronavirus (COVID-19) Infection Survey, UK Statistical bulletins
[3] Munday, Jarvis, Gimma, Wong, van Zandvoort, “Estimating the impact of reopening schools on the reproduction number of SARS-CoV-2 in England”, CMMID, number.cmmid.github.io
[4] Hobbs, Drobeniuc, Kittle, Williams, Byers, Satheshkumar, Inagaki, Stephenson, Kim, Patel, Flannery, “Estimated SARS-CoV-2 Seroprevalence Among Persons Aged <18 Years — Mississippi, May–September 2020,” CDC Morbidity and Mortality Weekly Report.
[5] Hyde, “Difference in SARS-CoV-2 attack rate between children and adults may reflect bias,” Clinical Infectious Disease, inacademic.oup.com
[6] “Children’s Task and Finish Group: update to 4th Nov 2020 paper on children, schools and transmission”
[7] Gurdasani, Alwan, Greenhalgh, Hyde, Johnson, McKee, et. al., “School reopening without robust COVID-19 mitigation risks accelerating the pandemic,” The Lancet
[8] Chernozhukov, Victor; Kasahara, Hiroyuki; Schrimpf, Paul. “The Association of Opening K-12 Schools and Colleges with the Spread of Covid-19 in the United States: County-Level Panel Data Analysis,” CESifo Working Paper No. 8929, March 2021.
[9] Vlachos, Hertegård, Svaleryd, “The effects of school closures on SARS-CoV-2 among parents and teachers,” PNAS
[10] Riley, Wang, Eales, Haw, Walters, Ainslie, Atchison, Fronterre, Diggle, Ashby, Donnelly, Cooke, Barclay, Ward, Darzi, Elliott, “REACT-1 round 9 final report: Continued but slowing decline of prevalence of SARS-CoV-2 during national lockdown in England in February 2021.”
[11] Vlachos, Hertegård, Svaleryd, “The effects of school closures on SARS-CoV-2 among parents and teachers,” PNAS ;
Lessler, Grabowski, Grantz, Badillo-Goicoechea, Metcalf, Lupton-Smith, Azman, Stuart, “Household COVID-19 risk and in-person schooling”
Forbes, Morton, Bacon, et. al. “Association between living with children and outcomes from covid-19: OpenSAFELY cohort study of 12 million adults in England,” BMJ Husby, Corn, Krause, “SARS-CoV-2 infection in households with and without young children: Nationwide cohort study”
[12] “Updated estimates of the prevalence of long COVID symptoms,” ONS
[13] Lessler, Grabowski, Grantz, et. al., “Household COVID-19 risk and in-person schooling”
[14] Riley, Wang, Eales, Haw, Walters, Ainslie, Atchison, Fronterre, Diggle, Ashby, Donnelly, Cooke, Barclay, Ward, Darzi, Elliott, “REACT-1 round 9 final report: Continued but slowing decline of prevalence of SARS-CoV-2 during national lockdown in England in February 2021,” Real-time Assessment of Community Transmission Findings”
[15] Prather, Marr, Schooley, McDiarmid, Wilson, Milton, “Airborne transmission of SARS-CoV-2,” Science.
[16] Van den Berg, Schechter-Perkins, Jack, Epshtein, Nelson, Oster, Branch-Elliman, “Effectiveness of three versus six feet of physical distancing for controlling spread of COVID- 19 among primary and secondary students and staff: A retrospective, state-wide cohort study”
[17] Gurdasani, Alwan, Greenhalgh, Hyde, Johnson, McKee, et. al., “School reopening without robust COVID-19 mitigation risks accelerating the pandemic,” The Lancet







