
Global health financing is collapsing just as demands on health systems are rising. As funding retreats and reform debates intensify, a deeper question emerges about who bears the costs, and whether today’s fixes risk creating lasting damage that will be difficult to reverse.
To say that the field of global health is in state of flux would be an understatement. Peaking at 80.3 billion USD in 2021, global health financing fell to 39.1 billion USD in 2025. This is not just a reduction by half in just four years, but also the lowest since 2013.
Funding cuts endanger large scale victories of the past twenty five years, including the progress toward universal immunization targets and the control of HIV/AIDS, tuberculosis and malaria through global initiatives, threatening millions of lives worldwide. Discussions on the way ahead have reignited the debate on the global health architecture and how to make it work better for all. Several reform proposals, focusing on ideas of regional autonomy, reducing external reliance, efficiency and equity, greater country ownership and the provision of global public goods, question the role and relevance of current global health institutions in correcting long-standing inequities, while advocating for a new way ahead.
The global health community is right in its unease that the current global health architecture requires addressing, and reforms are overdue. But finding a way forward will not be easy. Global health has currently become a lightning rod of frustration among a wide range of groups — all seem to be tired of it, but often for very different reasons. Funding cuts by leading donors, driven by rising nationalism and domestic security concerns, are matched by global health fatigue among recipient constituencies that increasingly view external financing as being at odds with their own priorities.
Taking stock of where we stand
With the withdrawal of the United States and other major funders, vertical programs especially those focusing on HIV/AIDS, tuberculosis and malaria have been severely impacted. Key global initiatives are also under strain. Gavi, the vaccine alliance, is currently managing to preserve the focus on a set of core essential pediatric vaccines, but new vaccine introductions - both in terms of scale and scope - will be at risk in the future.
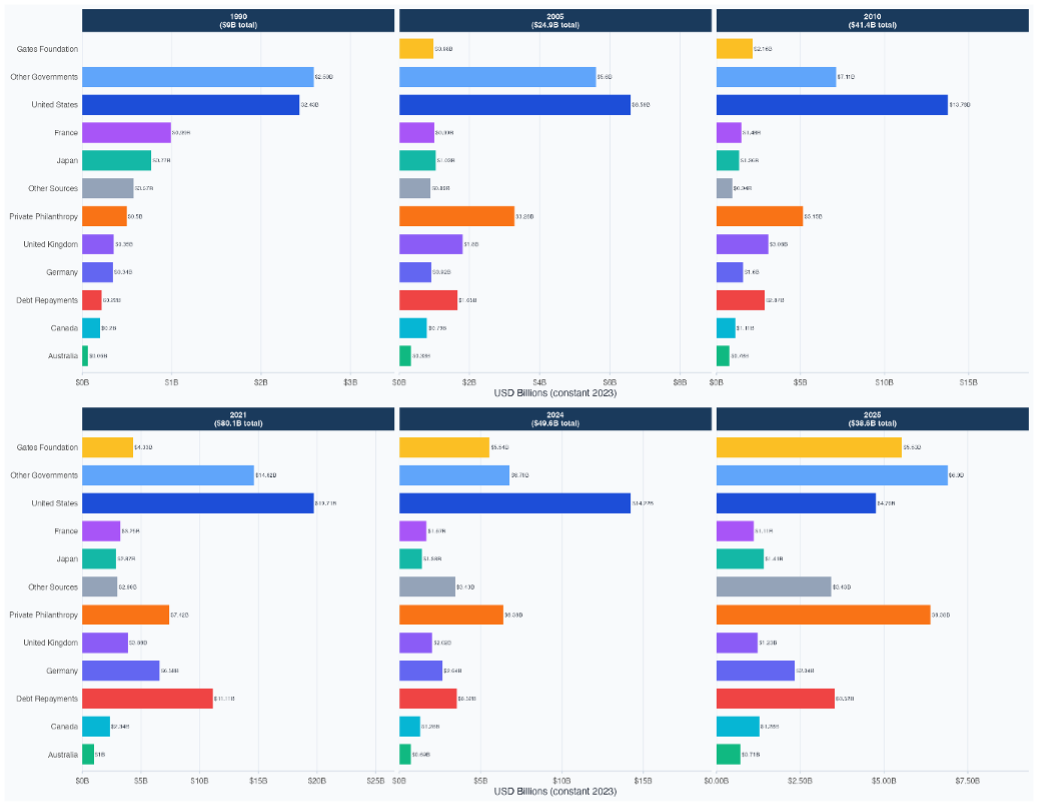
Figure 1: Development Assistance in Health: 1990 to 2025 Source: Author Calculations, IHME Data.
Other areas of global health at risk include: maternal mortality, pandemic preparedness and surveillance, sustained campaigns against the rise of anti microbial resistance, and neglected tropical diseases. The worst affected, however, is humanitarian support, with a fall in spending from USD 8 billion in 2024 to USD 5.8 billion in 2025, and a reduction in obligations $9.2 billion to $3.5 billion. As Figure 1 shows, the Gates Foundation and private philanthropy make the largest donors in 2025.
Has global health reform become populistic?
Presently, calls for a reframing health as a county-driven process are emerging from all across the spectrum: from constituents of donor countries who want a reduced aid footprint, to those arguing for a health systems approach to equip recipient countries to tackle their rising health needs, including domestic manufacturing and pandemic preparedness.
But discussions are more political than fact-based. For many donor countries, playing into the calls for ‘country ownership’ and ‘country owned’ is synonymous with low income countries stepping up to pay the bills for their own health budgets. For others, it signals the need to devise a system where global health financing is a means to augment domestic health financing. Mechanisms to enable this can take the form of co-financing arrangements, transition financing (with clear sunset clauses for end of donor funding), or other similar arrangements, such as Gavi’s eligibility, transitioning and co-financing policies. For yet others, it can mean that while financing of global health is outsourced, countries should have a greater say in how the programs are shaped.
In reality, the principles of ‘country led/ owned’, ‘country centric’, ‘one national health plan’, ‘one national budget’, ‘one monitoring framework’, ‘avoiding fragmentation’, ‘putting country needs first’ are not new. All of these have been voiced in yesteryear debates on global health - starting with 1978 WHO Alma Ata Declaration, to the 2005 Paris Declaration on Aid Effectiveness, to the Abidjan Declaration of 2024, among others.
So now the real question is whether we can move to a new stable state with the same principles? Will donors be able to hand over autonomy and empower local agencies in a system that has historically worked only through greater control through global organizations? Or is the ownership issue becoming a Trojan horse to shift the financing burden back to low income countries with little accountability for what is at stake?
From a pure numbers perspective, health spending in low income countries has been shrinking since the late 1970s. Starting in 1979, health spending in 29 of the poorest countries in sub-Saharan Africa declined by almost 25% as a result of austerity measures contained in the structural adjustment programs of the World Bank and the IMF. WHO’s Global Health Expenditure Database (GHED) shows that over the longer term, this trend has not recovered. Comparatively, while sub-Saharan Africa started out in a similar position as Asia in the early 2000s, countries in the region have not made the same kind of progress over the past two decades as in Asia (the latter spent 6% of their GDP on health, whereas the SSA countries spend a dismal 3%). Secondly, almost all low and low and middle income countries saw declines in governmental health spending in the period 2015-2019. Although the pandemic reinforced health funding to some extent, many if not most low income countries, especially sub-Saharan African countries, still lag far behind.
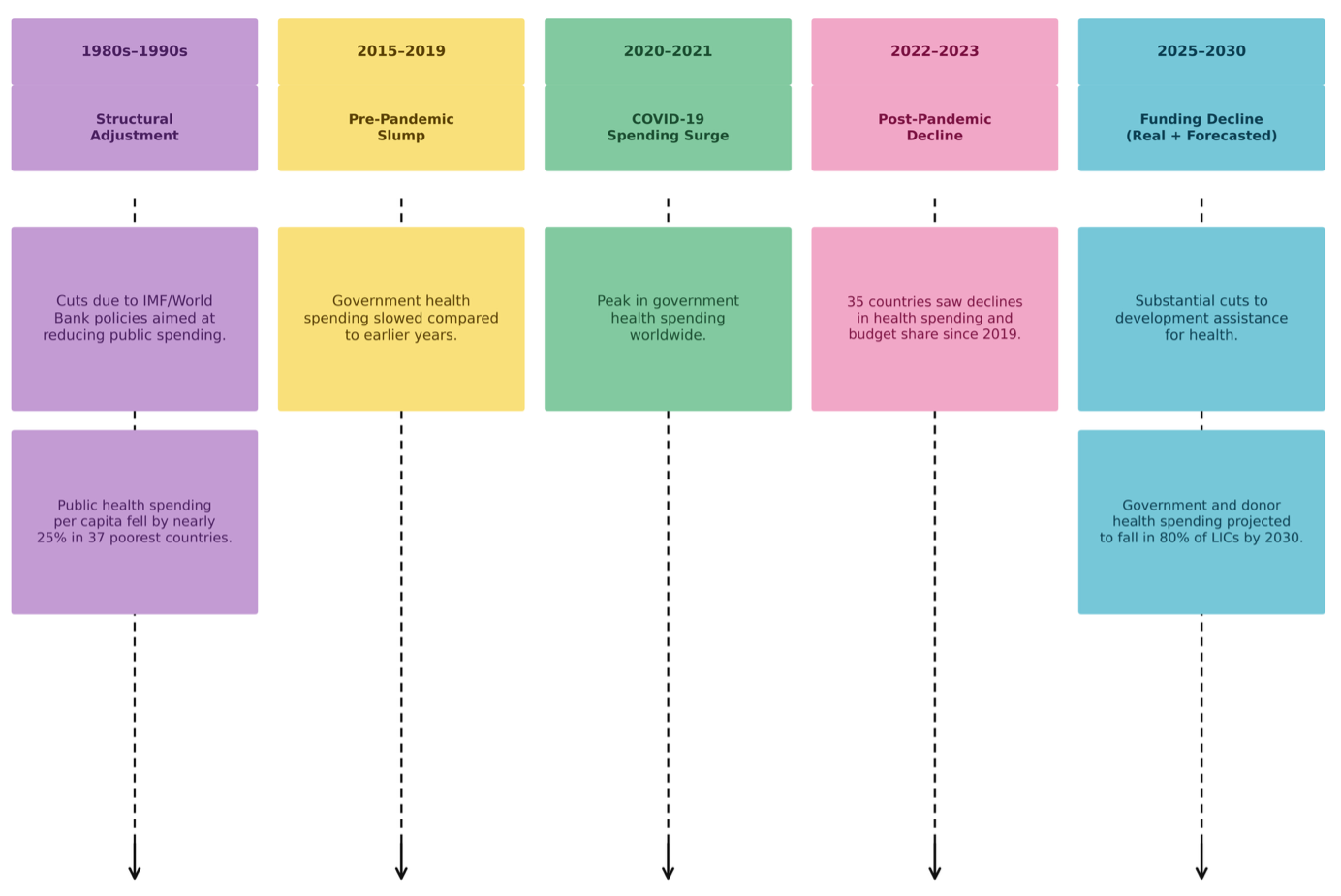
Figure 2: Health spending in low income countries: A historical overveiw
So, can a low-income country muster up enough sufficient domestic resources in this hard pressed global economy with across-the-board Overseas Development Assistance cuts, economic pressures, and food and fuel shortages to step up and spend more on health than it has done for several decades now?
The Real Cost: Hysteresis in Health systems
Hysteresis refers to the path dependency of a system and to how it reacts to temporary shocks even after the shock is removed. Closely linked to the concept of resilience (the ability to bounce back to the original state or move to a better one), it helps to showcase how cuts to health funding can have lasting, irreversible effects, long after the funding drop is reversed. When health systems are suddenly underfunded - like the current 51% drop in global health financing from 2021 to 2025 - they rupture in ways that make it harder to normalize again, as Figure 3 suggests.
Table 1 below explains some of the ways in which hysteresis sets in from the current funding crisis.
Table 1: How Hysteresis Works
Component | Impact | Hysteresis Effect |
Health workforce | Reduced vocational training and community programs, job cuts for technical health personnel. | Permanent exit of skills. Rebuilding skilled workforce will need years and massive investment. |
Infrastructure and supply chains | Cuts to cold-chain equipment and logistical infrastructure, mobile vehicles for supply delivery, warehouses, health management information systems, etc | Lack of maintenance, and eventual loss of health systems capital stock. |
Behavioral and epidemiological shifts | Lack of access to lifesaving medicines and interventions | Sudden lack of access leading to changes in community behavior, lack of trust in long term health programs, shifts in disease patterns with re-emergence of eradicated illnesses, emergence of drug resistant variants, and increase in health burdens. |
Loss of institutional memory | Loss of experienced personnel across the board. | Incapacity to run programs when funding is reinstated. |
The underfunding of humanitarian settings will have worse consequences not only because these catastrophes are presently going largely unnoticed. But also because fragile ecosystems such as those in Afghanistan, Gaza, Somalia, Sudan, Syria, and the Horn of Africa have persistent and urgent health needs and no reserves to recover in any reasonable manner.
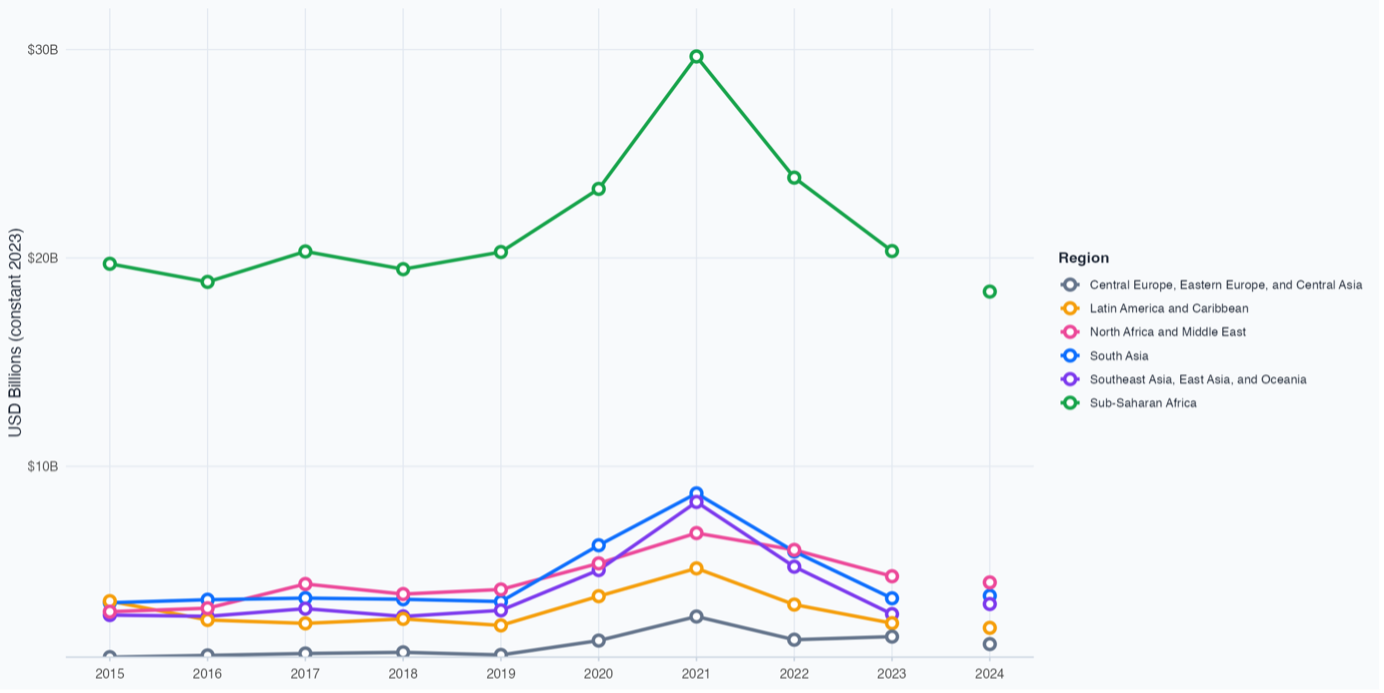
Figure 3: Global Health Financing by region, 2015-2025 Source: Author’s Calculations, IHME Data, 2025 projected figures not included.
What all of this means, in fact, is that without sufficient consideration of the real costs and who bears it, any discussion on reforming the global healthcare architecture will just become an attempt to wash our hands of it.



